When an Enlarged Prostate Becomes a Problem
The prostate is a small gland that sits below the bladder and surrounds the urethra — the tube that carries urine out of the body. As men age, the prostate often grows larger. This is called benign prostatic hyperplasia (BPH), and it’s extremely common.
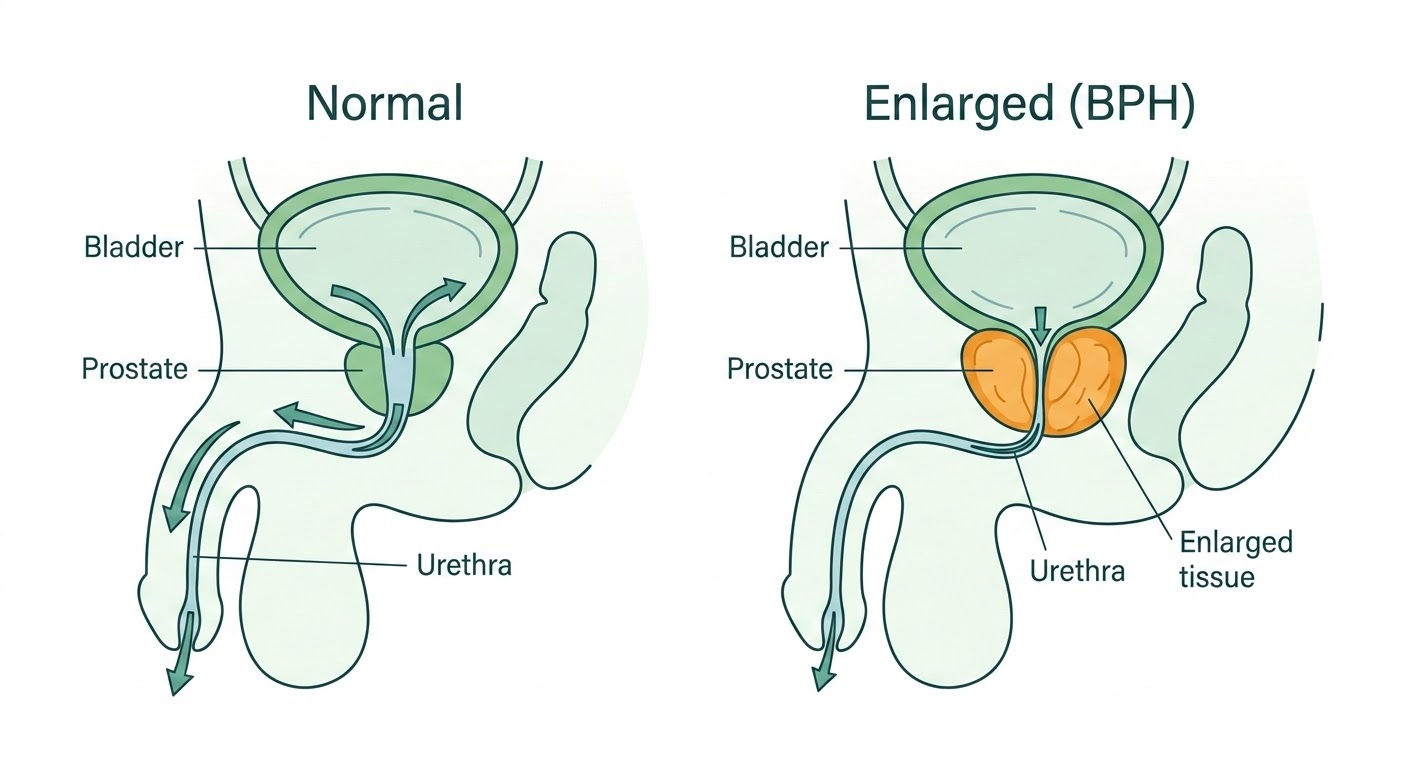
For many men, the growth is gradual and manageable with medication. But when the prostate becomes large enough to squeeze the urethra significantly, it can cause real problems: a weak or interrupted stream, the feeling that the bladder never fully empties, getting up multiple times at night, and in more advanced cases, an inability to urinate at all.
When medications are no longer enough, surgery to remove the obstructing tissue is the next step. The question is which approach.
What is GreenLEP?
GreenLEP — GreenLight Laser Enucleation of the Prostate — is a minimally invasive laser procedure that removes the enlarged portion of the prostate causing the blockage. A specialized laser fibre is passed through the urethra (no incisions are made), and the obstructing tissue is carefully separated from the outer shell of the prostate and vaporized.
The procedure uses the GreenLight XPS 180W laser — a well-established platform that many men in the GTA may have heard of in the context of laser vaporization (PVP). GreenLEP takes that technology further: rather than shaving tissue away from the surface, the laser is used to separate the entire blockage as a unit — the same principle as traditional open surgery, but done through the natural urinary passage with no cuts.
Most patients go home the same day or the following morning.
Who Is This For?
GreenLEP can be performed on prostates of any size — including very large glands of 200 grams or more — where standard approaches may struggle with the volume of tissue involved, and where open or robotic surgery would otherwise be the main alternative.
It may be appropriate when:
- Prostate medications are no longer controlling symptoms
- The bladder is not emptying properly, or you are unable to urinate at all
- Urinary infections or bladder stones keep coming back because of the blockage
- Blood thinners make other surgical options riskier
A Note About Bladder Function
Surgery removes the blockage. What it cannot do is repair a bladder that has lost its ability to squeeze. When obstruction has been present for a long time, the bladder muscle can weaken to the point where it no longer has enough tone to empty itself. In those cases, even reducing the prostate size may not help you fully empty — no operation, regardless of technique, will fully restore a strong stream.
This is assessed during the consultation. When the bladder is still working well, the results of surgery can be dramatic. When it isn’t, that conversation happens before any decision is made.
This is not a reason to delay seeing a specialist. It is a reason to be seen sooner, before irreversible changes occur.
Advantages of GreenLEP
Works at Any Size
Standard laser vaporization slows down as the prostate gets bigger — a very large gland requires far more time and energy. GreenLEP separates the blockage as a whole unit, so the approach scales to any size, including prostates over 200 grams.
Low Bleeding Risk
The GreenLight laser naturally seals blood vessels as it works, making bleeding during and after surgery substantially lower than with traditional approaches. This is especially important for men who take blood thinners and may not be able to stop them safely.
Urinary Control Preserved
Because the laser works along the prostate’s natural tissue plane, it avoids disturbing the muscle that controls urination. The risk of stress incontinence — leakage with coughing, sneezing, or physical movement — is less than 1%.
Some temporary urgency is normal in the first weeks as the bladder adjusts. This almost always settles.
No Incisions
Everything is done through the natural urinary passage. There are no cuts, no drains, and most patients go home the same day or the next morning.
A note about sexual function. There is approximately a 10% chance of experiencing weaker erections after surgery. Additionally, there is at least a 50% chance of losing the ability to ejaculate — semen passes backward into the bladder instead of forward (retrograde ejaculation), which is common after any prostate surgery that opens the bladder neck. This means the procedure may not be compatible with future fertility. These risks are discussed in detail during the consultation.
What about other laser enucleation techniques? You may have read about HoLEP (holmium laser enucleation) or ThuLEP (thulium laser). These are all well-established enucleation approaches endorsed by international guidelines, and they share the same core principle: separating the enlarged tissue from the outer prostate shell through the urethra. The laser platform and specific technique vary, but the concept is the same. During your consultation, Dr. Yan will explain why GreenLEP is the approach used in his practice.
What to Expect
Consultation
After your family doctor sends a referral, you’ll be seen in clinic. The visit includes a review of your symptoms, medications, and relevant tests. Bladder function is assessed to make sure surgery is likely to help. If GreenLEP is appropriate, the procedure, risks, and recovery are discussed in detail, and a surgical date is booked.
Day of Surgery
The procedure is performed under spinal or general anaesthesia at St. Joseph’s Health Centre. It typically takes 60–120 minutes depending on the size of the prostate. A catheter is placed at the end of the procedure. Most patients go home the same day or stay one night.
First Week
The catheter is removed within a few days to one week, depending on prostate size. Blood in the urine and a burning sensation when urinating are normal during the early recovery period. Most men are driving within a week and returning to light daily activity.
Full Recovery — Weeks to Months
Full recovery typically takes several weeks to a few months. Blood in the urine and burning with urination gradually resolve over this period. Urinary urgency and frequency are common as the bladder adjusts to the absence of obstruction. Most men notice a significant improvement in their stream well before full healing is complete. A follow-up visit confirms recovery is on track.
If you take blood thinners: Patients on anticoagulation may experience more bleeding during recovery and the healing process may take longer. Coming off blood thinners before surgery is preferred when possible. When stopping is not safe, bridging strategies and other options are discussed on a case-by-case basis.
Very large prostates: For men with a very large prostate, there is a possibility that a second GreenLEP procedure may be needed in the future if tissue regrows or if the initial procedure does not remove the full volume of obstruction.
Overactive bladder. In men who have had an enlarged prostate for a long time, the bladder itself may have become overactive. After surgery removes the blockage, the bladder may still be pushing hard — leading to frequent and urgent trips to the bathroom. If this is significant, medication may be helpful down the line.
The first step, however, is lifestyle modification:
- Limit total fluid intake to no more than 1.5 litres per day
- Avoid bladder irritants — alcohol, coffee, tea, carbonated drinks, citrus, salty foods, and fatty foods
- Stop drinking fluids 4–6 hours before bed, especially if nighttime symptoms are a problem
The Evidence
GreenLEP and the GreenLight laser platform are supported by randomized trials, large case series, and international guideline endorsement. The summaries below are for patients and referring physicians who want to look further into the data.
Endorsed by International Guidelines
Endoscopic enucleation of the prostate — including GreenLEP — is recommended by both the European Association of Urology and the American Urological Association as a size-independent surgical option for BPH.
The GOLIATH Trial
Thomas et al., European Urology, 2016 — 281 patients, 29 centres, 9 countries
The GOLIATH Trial
Thomas et al., European Urology, 2016 — 281 patients, 29 centres, 9 countries
The largest randomized trial comparing GreenLight XPS 180W laser vaporization to conventional TURP. 136 patients received GreenLight and 133 received TURP across 29 centres in nine European countries. GreenLight was noninferior to TURP on symptom scores (IPSS), peak urinary flow (Qmax), and freedom from complications at both 6 months and 2 years. The proportion of patients complication-free through 24 months was 83.6% for GreenLight versus 78.9% for TURP. Reductions in prostate volume and PSA were similar in both arms.
The GOLIATH trial evaluated laser vaporization (PVP). GreenLEP builds on the same 180W XPS platform with the added step of enucleation for larger glands.
View full abstract
Background: The GOLIATH study is a 2-yr trial comparing transurethral resection of prostate (TURP) to photoselective vaporization with the GreenLight XPS Laser System (GL-XPS) for the treatment of benign prostatic obstruction (BPO). Noninferiority of GL-XPS to TURP was demonstrated based on a 6-mo follow-up from the study.
Objective: To determine whether treatment effects observed at 6 mo between GL-XPS and TURP was maintained at the 2-yr follow-up.
Design, setting, and participants: Prospective randomized controlled trial at 29 centers in nine European countries involving 281 patients with BPO.
Intervention: Photoselective vaporization using the 180-W GreenLight GL-XPS or conventional (monopolar or bipolar) TURP.
Results and limitations: One hundred and thirty-six patients were treated using GL-XPS and 133 using TURP. Noninferiority of GL-XPS on International Prostate Symptom Score, Qmax, and freedom from complications was demonstrated at 6-mo and was sustained at 2-yr. The proportion of patients complication-free through 24-mo was 83.6% GL-XPS versus 78.9% TURP. Reductions in prostate volume and prostate specific antigen were similar in both arms and sustained over the course of the trial. Compared with the 1st yr of the study, very few adverse events or retreatments were reported in either arm. A limitation was that patients and treating physicians were not blinded to the therapy.
Conclusions: Twenty-four-mo follow-up data demonstrated that GL-XPS provides a durable surgical option for the treatment of BPO that exhibits efficacy and safety outcomes similar to TURP.
Thomas et al., Eur Urol 2016. DOI: 10.1016/j.eururo.2015.07.054
Randomized Trial in Large Prostates
Elshal et al., BJU International, 2020 — 182 patients, 3-year follow-up
Randomized Trial in Large Prostates
Elshal et al., BJU International, 2020 — 182 patients, 3-year follow-up
A randomized trial comparing three surgical approaches for large prostates (80–150 mL): GreenLight vapo-enucleation (GL.PVEP, 60 patients), holmium laser enucleation (HoLEP, 60 patients), and bipolar resection (TURIS, 62 patients). All three achieved significant and comparable symptom improvement (IPSS) at each follow-up point. GreenLight and HoLEP had shorter hospital stays, less blood loss, and fewer capsular perforations than TURIS. At 3 years, re-do surgery for recurrent obstruction was needed in 6.7% of GreenLight patients, 9.7% of TURIS patients, and 0% of HoLEP patients.
View full abstract
Objective: To compare transurethral resection in saline (TURIS), Greenlight laser vapo-enucleation of the prostate (GL.PVEP), and holmium laser enucleation of the prostate (HoLEP), for controlling lower urinary tract symptoms secondary to large benign prostatic hyperplasia (BPH) and to assess non-inferiority of 3-year re-treatment rates.
Patients and methods: Eligible patients with BPH (prostate size 80–150 mL) were randomly assigned to one of the intervention groups. Non-inferiority of re-treatment rate was evaluated using a one-sided test at 5% level of significance.
Results: At the time of analysis, 60 GL.PVEP, 60 HoLEP and 62 TURIS procedures were included. Perioperative parameters were comparable between groups; however, the operative time was longer in GL.PVEP vs HoLEP and TURIS, at a mean (SD) of 92 (32) vs 73 (30) and 83 (28) min (P = 0.005). There was a significantly higher rate of capsular perforation in TURIS group (five, 8%) compared to one (1.6%) in the GL.PVEP group and none in the HoLEP group (P = 0.01). There was a significantly longer hospital stay, catheter-time and higher rate of blood transfusion in the TURIS group. There was significant but comparable improvements in the International Prostate Symptom Score in three groups at different follow-up points. At 3 years, re-treatment for recurrent bladder outlet obstruction was required more after GL.PVEP and TURIS. More re-do surgeries for recurrent obstructing prostate adenoma was reported after GL.PVEP (four, 6.7%) and TURIS (six, 9.7%) than for HoLEP (none) (P = 0.04).
Conclusion: The perioperative outcomes of GL.PVEP and HoLEP surpassed that of TURIS for the treatment of large prostates, but with a significantly prolonged operative time with GL.PVEP. The three techniques achieve good functional outcomes; however, 3-year re-treatment rates following TURIS and GL.PVEP were inferior to HoLEP.
Elshal et al., BJU Int 2020.
GreenLEP Case Series — 120 Patients
Ferrari et al., Minerva Urol Nephrol, 2022 — median prostate 98.5 mL, 18-month follow-up
GreenLEP Case Series — 120 Patients
Ferrari et al., Minerva Urol Nephrol, 2022 — median prostate 98.5 mL, 18-month follow-up
A single-centre series of 120 patients undergoing en-bloc GreenLEP with early apical release. Median prostate volume was 98.5 mL (IQR 83–130). 37.5% were on antiplatelet or anticoagulant therapy. Peak urinary flow more than doubled (median 9 → 20 mL/sec, P<0.001) and symptom scores dropped dramatically (IPSS median 26 → 7, P<0.001) at a median follow-up of 18 months. Only 1 patient required a blood transfusion. After 12 months, 1 patient reported stress incontinence (1 pad/day) and 1 reported de novo urgency.
View full abstract
Background: Green Light laser enucleation of the prostate (GreenLEP) is an endoscopic treatment to treat bladder outlet obstruction in men with large prostate (>100 cc). Herein, we describe our GreenLEP series and describe its safety and efficacy.
Methods: Between February 2014 and April 2019, 120 patients from a single center underwent en-bloc GreenLEP with early apical release. All procedures were performed with the AMS XPS laser generator (set: 120 W for vaporization and 20 W for coagulation). Morcellation was carried out with the Wolf Piranha morcellator. Data concerning the pre-, intra- and postoperative outcomes were prospectively collected.
Results: The median age was 66.0 (IQR: 61.0–71.0) years; 37.5% of the patients were under antiplatelet/anticoagulant therapy, 15.0% had indwelling catheter history. The median prostate volume and the baseline PSA value were 98.5 mL (IQR 83.0–130.0) and 4.2 ng/mL (IQR: 3.2–6.8), respectively. The median operative and lasing time were 65.0 (IQR: 51.0–83.5) and 6.0 (IQR: 6.0–10.0) minutes, respectively. In the postoperative period 1 patient was transfused. The median follow-up was 18.0 (IQR: 12.0–39.5) months. All patients had significant improvement in uroflowmetry (median from 9 mL/sec [IQR 7.8, 11.0] to 20.0 [IQR 18.0, 22.0], P<0.001) and symptoms control (IPSS median score from 26.0 [IQR 22.0, 28.0] to 7.0 [IQR 6.0, 8.0], P<0.001) over time. After 12 months 1 patient complained of stress incontinence (1 pad/day) and 1 of “de novo” wet urgency.
Conclusions: En-bloc GreenLEP with early apical release is a safe and effective procedure even for large volume prostates. It allows us to limit the use of laser energy and shorten the operating times with stable and satisfactory long-term outcomes.
Ferrari et al., Minerva Urol Nephrol 2022.
GreenLight vs HoLEP — Systematic Review Beyond 5 Years
Yim et al., 2025 — 25 studies, 180W model comparable to HoLEP at 5 years
GreenLight vs HoLEP — Systematic Review Beyond 5 Years
Yim et al., 2025 — 25 studies, 180W model comparable to HoLEP at 5 years
A systematic review of 25 studies comparing long-term (≥5 year) outcomes of GreenLight PVP and HoLEP. HoLEP demonstrated durable outcomes with low reoperation rates (mean 4.1%) at a mean follow-up of 7.3 years. Earlier GreenLight models (80W/120W) had higher reoperation rates (mean 12.6%), but three studies examining the current 180W XPS model showed superior durability comparable to HoLEP at 5 years. Longer-term data beyond 10 years for the 180W model is not yet available.
View full abstract
Objectives: This study aimed to compare long-term (≥5 years) functional outcomes and reoperation rates following holmium laser enucleation of prostate (HoLEP) vs GreenLight photoselective vaporisation of prostate (GLPVP).
Methods: MEDLINE, Embase and Cochrane databases were searched from inception to December 2023. Included were randomised controlled trials (RCTs), cohort studies and case series studying HoLEP and/or GLPVP, where functional outcomes and reoperation rates were reported. Studies with <5-year follow-up were excluded.
Results: Of 3047 records identified, 25 were eligible, including two RCTs, two cohort studies, one cross-sectional study and 20 case series. HoLEP demonstrated long-term durability of outcomes and low reoperation rates (mean 4.1%, range 2.0%–6.3%) at a mean follow-up of 7.3 years. GLPVP also had durable outcomes at 5-year follow-up, but inconclusive evidence for improvements at 10 years. Reoperation rates were also higher (mean 12.6%, range 3.8%–33.3%). Three studies examined the 180-W GLPVP model at 5 years showed superior durability to earlier 80-W/120-W models.
Conclusions: Current evidence suggests that HoLEP provides significantly greater functional improvements and a lower reoperation rate when compared with the GLPVP 80-W/120-W model at 5-year follow-up. The 180-W model is comparable with HoLEP based on limited data at 5 years, but there is a lack of data beyond 10 years for longer-term functional outcomes.
Yim et al., 2025. DOI: 10.1002/bco2.483
Is This Right for You?
Not every man with a large prostate needs surgery, and not every man who needs surgery is best served by GreenLEP. The consultation is where that is worked out — reviewing the symptom history, the bladder function, the anatomy, the medications, and what you actually want from the outcome.
A referral from your family physician is the first step. From there, the assessment is straightforward.
If You Are in Retention or Catheter-Dependent
Patients who are unable to urinate on their own or who are dependent on a catheter are prioritized for both consultation and surgical booking. If this applies to you, please ask your family physician to indicate it on the referral so we can expedite the process.
How to Refer
Family Physicians
Fax referrals are preferred and accepted at 416-767-2403.
You may also email Dr. Yan’s secretary, Cathy Zagouris, at cathy.zagouris@unityhealth.to.
Patients in retention or catheter-dependent — please flag on referral for expedited booking.
Ocean eReferral is pending and will be available soon.
Patients
A referral from your family physician or nurse practitioner is required. Please ask them to fax or email a referral to Dr. Yan’s office at St. Joseph’s Health Centre.
